

Is Your Shoulder Just Stiff, Or Is It Frozen?
In the beginning, you’ll feel pain at the front or side of the shoulder which can be a sudden or a gradual onset. Depending on the intensity of your pain, it can often cause difficulty in sleeping or wake you up in the middle of the night. Overtime, you start noticing that you are losing freedom of movement in the shoulder. This is when it hits you that the shoulder problem is serious, and you should seek consultation with a healthcare professional.
In this article, we have a chat with Senior Physio, Anson Wong and Dr Ang from Centurion Orthopaedic Centre to discuss all things Frozen Shoulder. You can find Dr Ang at https://www.coc.sg/
What Is Frozen Shoulder?
Frozen shoulder, AKA adhesive capsulitis, was first introduced in 1934 by Codman. He described the condition as “hard to define, difficult to treat and hard to explain”, which remains true today.
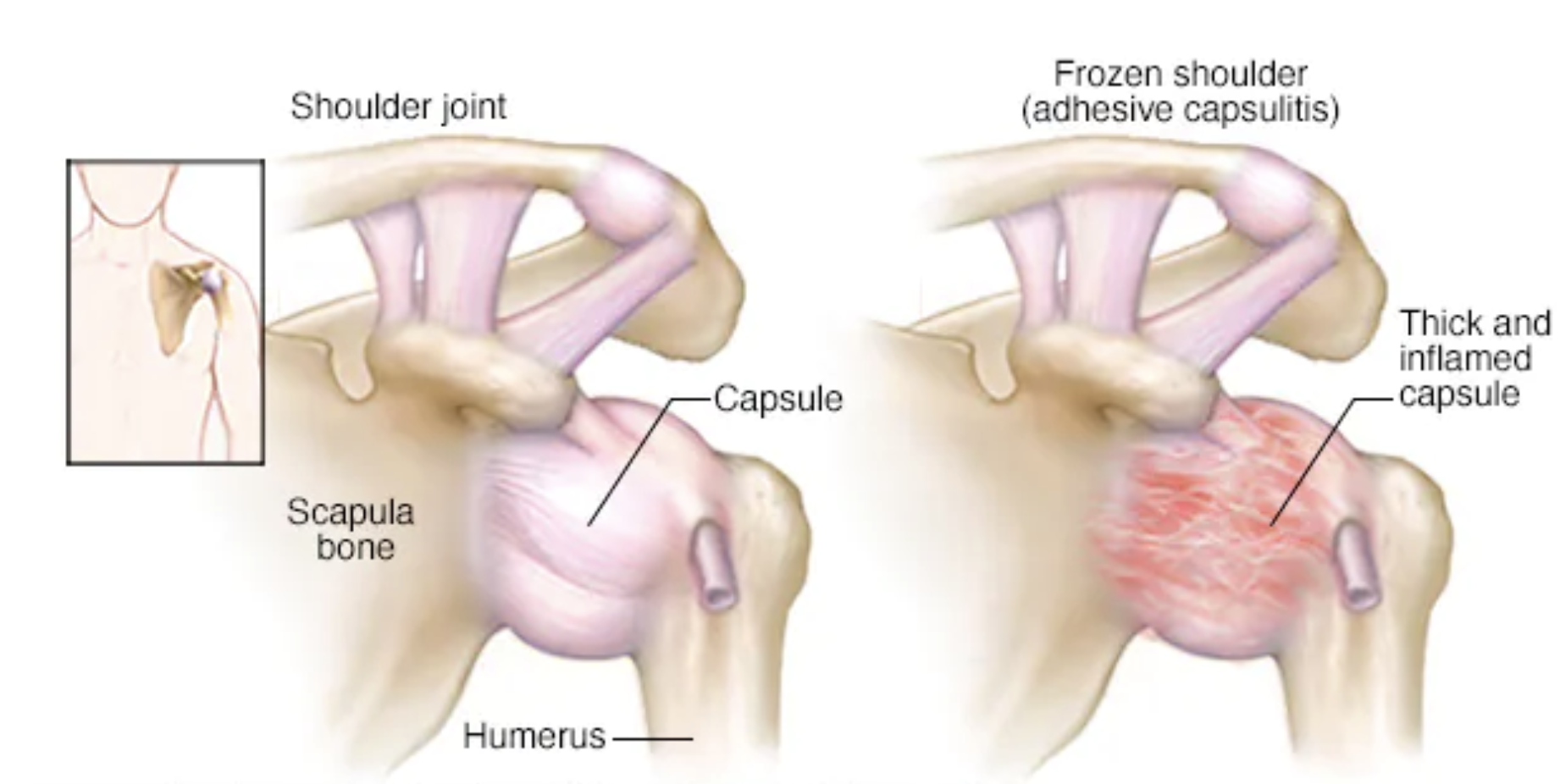
We know that most of the structural changes with frozen shoulder happen at the front of your shoulder. While the immune system, inflammatory process, and fibrosis each plays a role in the disease progression, we still cannot determine to what extent each component contributes to frozen shoulder.
With frozen shoulder, contraction of the shoulder joint occurs. Your shoulder joint capsule becomes thickened, fibrosed and you lose the volume of space within the shoulder joint. This can result in severe disruption to your lifestyle, causing you difficulty at work or going through simple daily activities.
Classification Of Frozen Shoulder
Traditionally, frozen shoulder flows in 3 stages:
1. Freezing phase: The onset of shoulder pain with gradual loss of shoulder movement.
2. Frozen phase: gradual reduction of pain, with stiffness plateauing in both active and passive shoulder range of motion.
3. Thawing phase: The gradual improvement of shoulder mobility.
However, it is important to recognise that the disease process is a continuum rather than having well-defined phases. Dr Ang personally prefers categorising frozen shoulder into 2 groups:
- Pain predominant
- Stiffness predominant
This classification is not only simpler but easier for patients to associate with their symptoms, and most importantly, more practical in determining the treatment strategy.
To understand more about the causes, diagnosis, and treatment of frozen shoulder, we had a chat with Dr Ang Chia Liang
Let’s have a quick summary of what both Dr Ang and Anson discussed about!
What Causes Frozen Shoulder?
In many cases, the cause is obscure. Common risk factors include having an untreated shoulder condition such as shoulder impingement or tendon damage, or recent hospitalisation with prolonged immobility of the shoulder. Frozen shoulder occurs commonly in the 40s to 50s age-group and diabetics are at a higher risk of developing the condition.
How To Diagnose Frozen Shoulder?
Frozen shoulder is diagnosed primarily through a clinical assessment by the Orthopaedic specialist or through a comprehensive assessment by your physio. They will ask questions about your shoulder and carry out a physical examination, checking the range of motion of your shoulder to detect whether there may be other coexisting shoulder problems.
A common symptom of frozen shoulder is the loss of both active and passive range of motion in the shoulder. This means that you are unable to lift your shoulder past a certain height, even with any form of assistance. X-rays and Magnetic Resonance Imaging (MRI) scans are useful tests to confirm the diagnosis as well as examine for other common related conditions of the shoulder, such as impingement and rotator cuff tear.
Treatment For Frozen Shoulder
In the first 2-3 months of acute frozen shoulder, when the pain is most significant, a steroid injection to the shoulder is a very good way to reduce pain and inflammation as well as help with recovery. This then allows the patient to undergo physiotherapy without too much pain. It is important to understand that when used in this way, the steroid is meant to treat the condition and not merely as a ‘pain-killer’.
In some cases where improvement is slow and is causing the patient significant discomfort, a safe and straight-forward key-hole treatment helps patients regain movement of the shoulder immediately. This is called Arthroscopic Capsular Release and is a Day Surgery procedure.
Let’s Bust A Myth: Frozen Shoulder Can Be Recovered On Its Own
There is a notion that you can recover from frozen shoulder without supervised treatment. However, recent scientific studies have shown that this is false. While the average duration for frozen shoulder ranges from 1 to 3.5 years, there are patients who still suffer from mild to moderate symptoms at 7 years.
The belief that frozen shoulder can be recover on its own can cause one to delay or refuse treatment. Many patients suffering from frozen shoulder undergo a punishing recovery journey even though treatment is readily available. Improvement in frozen shoulder occurs early, but, it will gradually decrease with time, resulting in chronic limitation that can last for multiple years. Thus, it is extremely important for you to get frozen shoulder diagnosed and treated as early as possible!
Written By: Anson Wong And Dr Ang Chia Liang
About Anson – Senior Physiotherapist, B.Sc. (Hons) Physiotherapy (MY)
Anson has 9 years of experience in physiotherapy, and specialises in musculoskeletal and sports injury rehabilitation. His main areas of focus include the shoulders, knees, and ankles. He is certified in dry-needling and is also a Certified Mulligan Practitioner.
About Dr Ang Chia Liang – Orthopaedic Surgeon, MBBS, MRCS (Ed), ECFMG, MMed (Ortho), FRCSEd (Ortho)
Dr Ang has more than 19 years of Orthopaedic experience. He has expertise in knee, hip, and shoulder conditions, sub-specialising in Minimally Invasive treatment of joint conditions, joint replacements, and fractures. Dr Ang has also performed over 6000 orthopaedic surgeries and more than 1500 knee surgeries.